Designed to Perform
The Medartis Olecranon System 2.8 offers a range of plates with innovative fixation concepts that may help reduce soft tissue irritation and therefore reduce the rates of hardware removal surgeries. [1]
[1] A. Ellwein, K. Argiropoulos, R.-O. DeyHazra, M.-F. Pastor, T. Smith, H. Lill “Clinical evaluation of double-plate osteosynthesis for olecranonfractures: A retrospective case-control study” Orthopaedics & Traumatology: Surgery & Research, 2019, 105 (8); 1601-1606
Fixation Options
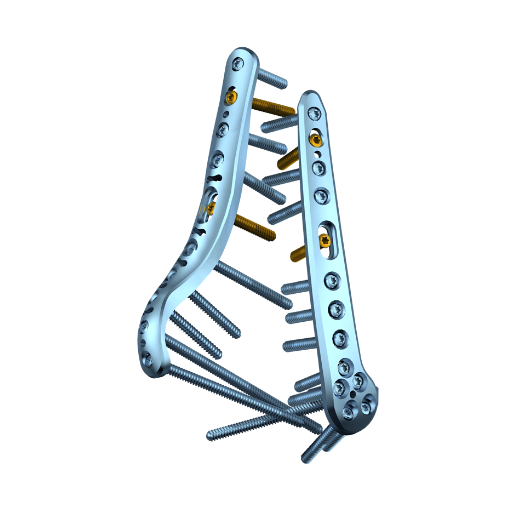
The low profile 2.8 TriLock Olecranon Double Plates are designed to fix complex olecranon fractures without interfragmentary support. Their innovative lateral positioning allows for muscular soft-tissue coverage and an increased amount of screws to hold small proximal fragments. [2]
The 2.8 TriLock olecranon tension plate was developed as a replacement of the classic tension band wiring. The low-profile plate is very thin entailing limited hardware prominence [3] and can withstand tensile forces. It is indicated for fractures and osteotomies of the proximal ulna with interfragmentary support.
[2] F.C. Wagner, M. Jaeger, C. Friebis, D. Maier, C. Ophoven, T. Yilmaz, N.P. Südkamp, K. Reising, “Low-profile double plating of unstable osteoporotic olecranon fractures: a biomechanical comparative study”, J Shoulder Elbow Surg, 2021, 30(7); PP1519-1526
[3] D. Gruszka, C. Arand, T. Nowak, S.O. Dietz, D. Wagner, P. Rommens, «Olecranon tension plating or olecranon tension band wiring? A comparative biomechanical study», International Orthopaedics (SICOT), 2015, 39:955-960



TriLock Olecranon Curved Double Plates 2.8

Highlights
-
Low plate profile and high rotational stability due to biomechanically favourable posterolateral and posteromedial plate position
-
Plates can be covered with soft tissue (anconeus muscle und flexor carpi ulnaris muscle), thereby reducing the occurrence of wound healing problems and the likelihood of hardware removal [1,2]
-
High number of screw options enables stable fixation particularly of small proximal fragments [2]
-
High primary stability due to screw position orthogonally to the direction of the pulling force of the triceps brachii muscle [2]
-
Easy bending to adapt to the individual anatomy of the patient
TriLock Olecranon Straight Double Plates 2.8

Highlights
-
Distal plate position spares the triceps tendon insertion
-
Low plate profile and high rotational stability due to biomechanically favourable posterolateral and posteromedial plate position
-
Plates can be covered with soft tissue (anconeus muscle und flexor carpi ulnaris muscle), thereby reducing the occurrence of wound healing problems and the likelihood of hardware removal [1,2]
TriLock Olecranon Tension Plate 2.8

Highlights
-
Developed as a replacement of the classic tension band wiring
-
The low-profile plate is very thin entailing limited hardware prominence [3] and can withstand tensile forces
-
Two cross-fracture lag screws provide primary compression and fixation [3]
-
Uniform and controlled compression of the fracture with lag screws allows for mobilization as early as possible [3]
-
Solid anchoring of the tension relief even in osteoporotic bone reduces the risk of fracture dislocation [3]
Screws

Locking
2.8 TriLock Screws,
HexaDrive 7

Non - Locking
2.8 Cortical Screws,
HexaDrive 7

Lag Screws
2.8 Lag Screws,
HexaDrive 7
Technological Milestones in Osteosynthesis
TriLock
Multidirectional and angular stable locking, screws can pivot freely by ± 15° in all directions
TriLockPLUS
TriLockPLUS screw holes offer the advantage of locking and compression in one step
HexaDrive
Simplified screw pick-up due to self-holding system
Designed to Organize

- Compact system
- Easy to use
- Lightweight components
- Validated cleaning and sterilization of the implants
Documentation
Results
- Elbow System 2.0, 2.8 – Surgical Technique 22.01.2024 7 MB Surgical Technique Upper Extremities English
- APTUS Ordering Catalog/Bestellkatalog/Catalogue (High Resolution) (Version 0, MDR) 18.01.2024 22 MB Ordering Catalog Upper Extremities English
- APTUS Ordering Catalog/Bestellkatalog/Catalogue (Low Resolution) (Version 0, MDR) 18.01.2024 16 MB Ordering Catalog Upper Extremities English